What Does Lower Crossed Syndrome Feel Like? To be honest, due to modern lifestyles and work patterns, lower crossed syndrome has become increasingly common—yet many people are not even aware that they have it.
For example, some people deliberately push their hips back to create the appearance of glute development, while others notice a protruding lower abdomen and assume it is simply due to excess body fat, leading them to focus only on weight loss. In reality, these are often symptoms of lower crossed syndrome rather than purely aesthetic or fat-related issues.
So what are the causes of lower crossed syndrome?
How is lower crossed syndrome characterized, and which overactive muscles are involved in this postural imbalance?
In today’s article, we will break down each of these questions step by step.
What Is Lower Crossed Syndrome?
Lower crossed syndrome, also known as pelvic girdle crossed syndrome, is a postural imbalance involving the pelvis, hips, and lower spine. It is characterised by a specific pattern of muscle tightness and muscle weakness that pulls the pelvis away from its neutral position.
Understanding this pattern is essential before attempting to “fix” it.
Lower Crossed Syndrome Symptoms
Common symptoms include:
- Anterior pelvic tilt
- Increased lumbar lordosis (exaggerated lower-back curve)
- Leg rotation (In-Toeing or Out-Toeing)
- Knee hyperextension
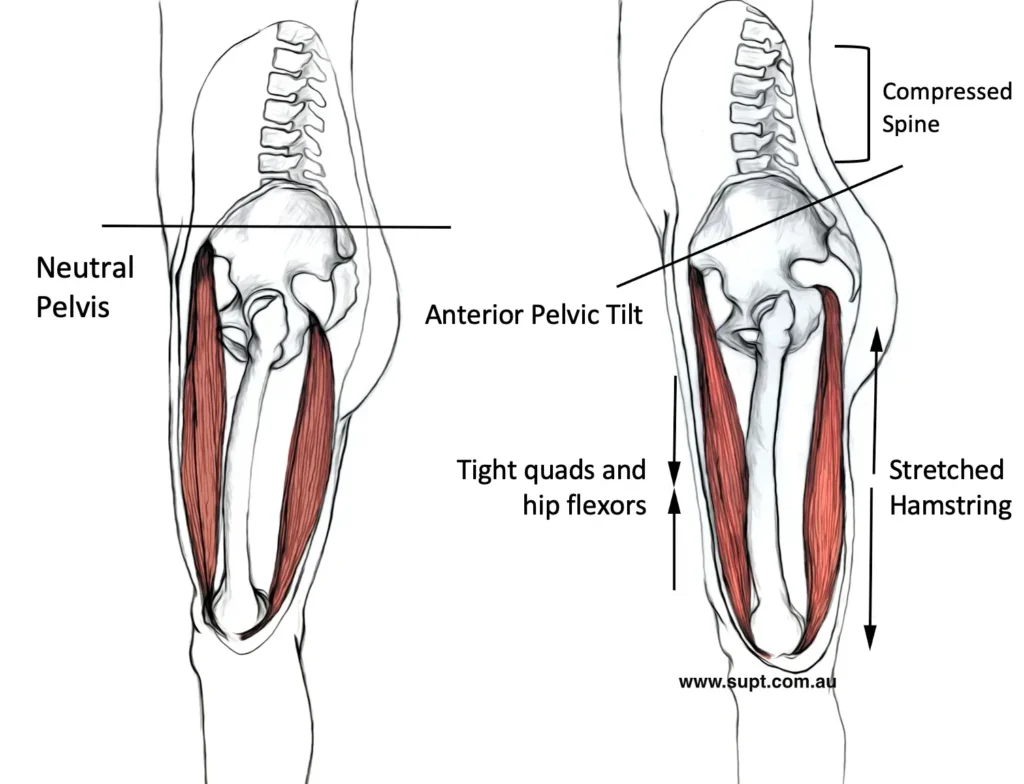
1) Anterior Pelvic Tilt (APT)
The most recognisable sign of lower crossed syndrome is anterior pelvic tilt. Simply put, the pelvis tilts forward. A helpful visual is to imagine a water bottle tipping forward as it pours water—this closely resembles the orientation of the pelvis in anterior tilt.
As the pelvis tilts forward, the lumbar spine compensates by increasing its natural curve, a condition known as increased lumbar lordosis. When this posture is maintained over time, the lower back often feels persistently fatigued or tense.
Recommend:What is an ‘Anterior Pelvic Tilt’ and How to Correct it.
2) Leg Rotation
Leg rotation refers to a standing or walking posture in which the toes do not point straight ahead.
- In men, this commonly presents as a toe-out posture.
- In women, it may present as toe-in posture.
This pattern is usually linked to hip joint stability and neuromuscular control, rather than isolated tightness in the lower leg..”
3) Knee Hyperextension
Knee hyperextension occurs when the knee extends beyond its normal anatomical position of 180 degrees.
A simple self-check is to observe the back of the knee. If the popliteal area visibly protrudes backward when standing, knee hyperextension is likely present.
In everyday activities such as standing, the knee typically bears only approximately one times bodyweight, so hyperextension may not cause immediate problems. However, during resistance training—especially squat-based movements—the knee can experience multiple times bodyweight, significantly increasing the risk of long-term joint stress and injury.
Lower Crossed Syndrome Overactive Muscles
One of the defining features of lower crossed syndrome is abnormal pelvic positioning. Besides anterior pelvic tilt, the pelvis may also adopt a posterior tilt, while the optimal position is referred to as a neutral pelvis.
Both anterior and posterior pelvic tilt can lead to muscular tightness, but in different muscle groups.
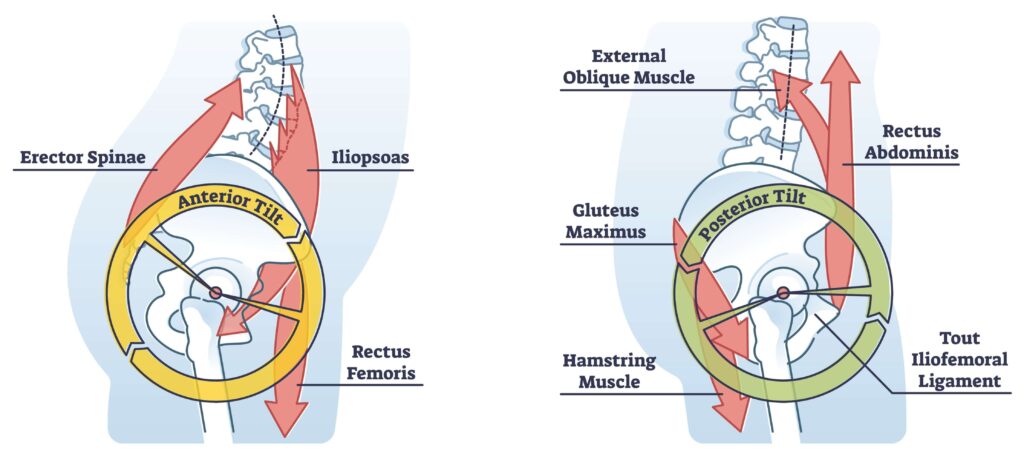
Muscles Commonly Tight in Anterior Pelvic Tilt
- Erector spinae
- Iliopsoas
- Rectus femoris
The erector spinae tend to pull the pelvis upward and backward, while the iliopsoas and rectus femoris exert a downward pull from the front of the body. The combined effect of these opposing forces results in anterior pelvic tilt.
Muscles Commonly Tight in Posterior Pelvic Tilt
- Gluteus maximus
- Hamstrings
- Rectus abdominis
- External obliques
In this case, the gluteus maximus and hamstrings pull the pelvis downward from behind, while the rectus abdominis and external obliques pull upward from the front.
Lower Crossed Syndrome Causes
The most common contributing factors include:
- Weak abdominal musculature (including special cases such as a protruding belly and pregnancy)
- Wearing high heels frequently
- Psychological and behavioural factors
Weak Abdominal Musculature
When sitting, the abdominal muscles are largely inactive. Prolonged sitting therefore leads to reduced core function. At the same time, anterior pelvic tilt reduces the upward stabilising force that the abdominal muscles should provide.
Over time, this imbalance contributes to the development of lower crossed syndrome.
However, two special populations should be considered separately: pregnant women and individuals with a protruding abdomen due to excess visceral fat.
In both cases, the abdominal muscles are lengthened and lose their ability to function effectively. This differs from the typical sedentary pattern, where the core is simply undertrained.
That said, pregnancy and a protruding belly are not identical:
During pregnancy, postural changes are largely temporary and occur due to physiological demands. After childbirth, posture often returns closer to normal without intervention. For this reason, posture correction during pregnancy is usually unnecessary unless anterior pelvic tilt persists postpartum.
A protruding belly caused by excess visceral fat shifts the body’s centre of mass forward. In this scenario, posture assessment and corrective training are often ineffective until body fat is reduced. Once fat loss occurs and the centre of mass moves back toward the lumbar spine, reassessment becomes meaningful.
Wearing High Heels Frequently
Wearing high heels frequently causes two major biomechanical issues.
First, high heels significantly alter load distribution in the feet. Under normal conditions, body weight is shared across three contact points: two in the forefoot and one in the heel. High heels shift a disproportionate amount of load onto the forefoot, and the higher the heel, the more pronounced this shift becomes.
Second, high heels force a postural compensation. Because the shoes tilt the body forward—similar to standing on an inclined surface—the body cannot remain balanced by leaning forward. Instead, the upper body stays relatively vertical while the pelvis tilts anteriorly and the trunk subtly shifts backward.
This creates the visual impression of an upright or “elegant” posture. Mechanically, however, the effect mirrors anterior pelvic tilt: increased lumbar lordosis and exaggerated glute projection. Over time, this posture contributes to pelvic alignment issues and excessive tightness in the calf muscles.
Psychological Factors
Psychological and behavioural factors may seem surprising, but they are not uncommon—particularly among office workers.
The gluteal region consists of both muscle and fat. Maintaining a round, firm appearance requires sufficient muscle mass, which typically demands significant resistance training. The gluteus maximus is the largest single muscle in the human body and is minimally activated during everyday walking.
A typical sedentary routine—long hours of sitting, commuting, and screen time—provides little stimulus for glute development. Over time, glute muscle mass may decrease while fat accumulation increases, leading to a sagging appearance.
To compensate visually, some individuals subconsciously exaggerate anterior pelvic tilt, increasing lumbar curvature and pushing the glutes backward. The positive aspect is that once glute strength improves through proper training, this compensatory posture often diminishes naturally.
What Does Lower Crossed Syndrome Feel Like?
Increased Lumbar Stress
From a biomechanical perspective, abnormal pelvic tilt increases stress on the lumbar spine and knee joints, particularly around the L5 vertebra and S1 (sacrum).
With neutral standing posture as a baseline (pressure = 100), sitting increases lumbar pressure to approximately 140. Both anterior and posterior pelvic tilt increase this pressure even further, which helps explain the high prevalence of lower back discomfort.
Protruding Lower Abdomen
Anterior pelvic tilt alters spinal curvature and diaphragm position, pushing internal organs downward and forward into the abdominal cavity. This creates a protruding lower abdomen that is not directly related to body fat.
This explains why some individuals with relatively low body fat still experience a visible lower belly bulge—and why fat loss alone often fails to correct it.
Sagging Glutes
Chronic anterior pelvic tilt places the gluteal muscles in a lengthened position. Over time, reduced activation and increased fat storage can produce a sagging appearance.en leads to poorer activation and fat accumulation, making the glutes look saggy over time.
Training Problems Associated With Lower Crossed Syndrome
Although anterior pelvic tilt may have limited impact on daily life, poor core function can significantly affect training performance.
Straight-Leg Raises
Straight-leg raises are commonly assumed to train the abdominal muscles. In practice, the primary movers are often the hip flexors, particularly the iliopsoas and rectus femoris.
According to exercise science principles, the target muscle of a movement is the muscle responsible for the concentric contraction.
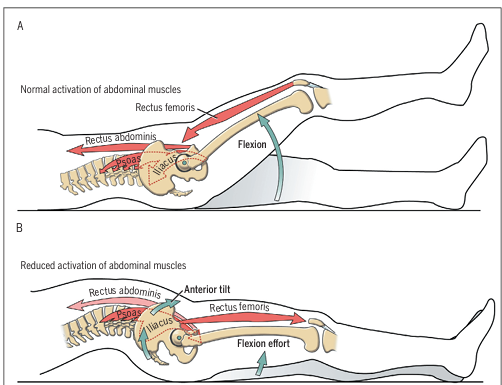
When core stability is adequate, the iliopsoas, rectus abdominis, and external obliques contract first to stabilise the pelvis. Once stability is achieved, the rectus femoris lifts the legs.
In individuals with anterior pelvic tilt, the rectus abdominis is often weak and unable to stabilise the pelvis. As the legs attempt to lift, the pelvis moves first. Due to the long lever arm of the legs, the rectus femoris pulls downward on the pelvis, increasing lumbar lordosis and spinal stress—often resulting in lower back pain.
Sit-Ups
Sit-ups follow a similar pattern. Only the first ~30 degrees of trunk flexion meaningfully involve the abdominal muscles. From approximately 30 to 90 degrees, hip flexors dominate the movement.
If the iliopsoas and rectus femoris are tight, they exert a downward pull on the lumbar spine. Even small changes in muscle activation order can reverse movement mechanics and increase injury risk.
Bent-Over Movements
Bent-over exercises require alignment of the head, upper back, and sacrum, with the core providing stability. In individuals with anterior pelvic tilt and weak abdominal control, the lumbar spine is already under excessive stress. Training in this state is inefficient and increases the likelihood of injury.

{kind=link}